
India has a diabetes problem that is difficult to overstate.
Over 100 million Indians are currently living with type 2 diabetes — the highest absolute number of any country in the world. Tens of millions more are in the pre-diabetes zone, moving toward it without knowing. Obesity rates are climbing. Cardiovascular disease is striking younger. The lifestyle epidemic that we have written about before is not a future threat. It is happening now, in cities, in offices, in people in their 30s and 40s who had no reason to expect it yet.
Into this context, two drugs have arrived that genuinely deserve the word miracle: Ozempic, Mounjaro and Wegovy.
We want to be clear about this before anything else: these are remarkable drugs. They are saving lives. And in India specifically, where the metabolic disease burden is enormous and growing, their potential impact is significant. This blog is not an argument against them.
It is an argument for asking the next question — the one that most people, and most prescriptions, are not yet asking.
What These Drugs Are and How They Work

Ozempic and Wegovy are both brand names for the same active ingredient: semaglutide, developed by Danish pharmaceutical company Novo Nordisk. The story of how it came to exist is worth knowing.
In the early 1990s, researchers discovered that a hormone called GLP-1 — glucagon-like peptide-1 — released naturally by the gut after eating, played a significant role in regulating blood sugar. It stimulated insulin secretion, suppressed glucagon, and signalled the brain that the body was full. The problem was that natural GLP-1 has a half-life of barely one to two minutes in the bloodstream — far too short to be therapeutically useful.
Novo Nordisk researchers spent years engineering a synthetic version that would survive long enough to matter. After testing thousands of combinations of molecular modifications, they developed semaglutide — a compound that shares 94% structural similarity with human GLP-1 but has a half-life of approximately one week, allowing it to be administered as a once-weekly injection.
Ozempic was approved for medical use in the US in 2017. When diabetic patients in early trials began showing unexpected and significant weight loss alongside blood sugar improvements, researchers pursued higher doses specifically for obesity treatment. The result was Wegovy — the same molecule at a higher dose, approved for weight management.
In a clinical trial for Wegovy, patients who received a once-weekly injection for two years experienced, on average, a 14.8% reduction in weight compared to 2.4% reduction with placebo. Some patients on the highest doses lost more than 20% of their total body weight.
Beyond weight loss, GLP-1 receptor agonists have shown additional benefits including lowering blood pressure, improving lipid disorders, improving fatty liver disease, and reducing the risk of heart disease and kidney disease.
For a country like India — where diabetes, hypertension, and cardiovascular disease are converging at younger and younger ages — this is genuinely transformative medicine.
The Side Effects People Know About

The most common adverse effects include nausea, vomiting, abdominal pain, constipation, and diarrhea — nearly one-fifth of all patients in clinical trials experienced nausea. These are typically mild to moderate and tend to reduce over time as the body adjusts to the medication.
There are more serious but rarer risks. Semaglutide carries a boxed warning for thyroid C-cell tumours observed in rodents, though whether this applies to humans remains unknown. Cases of gastroparesis and bowel obstruction have also been reported.
These are the risks that most prescriptions and most conversations address. They are real and worth knowing.
But there is another risk that is receiving far less attention — one that connects directly to everything we have written about muscle health, sarcopenia, and the specific vulnerability of Indian bodies.
The Muscle Loss Nobody Is Talking About
When the body loses weight rapidly — through any mechanism, drug-assisted or otherwise — it does not draw exclusively from fat stores. It draws from multiple tissue sources simultaneously. This is basic physiology. The question with semaglutide is: how much of the weight being lost is fat, and how much is muscle?
The data is striking.
In the 68-week STEP-1 trial of semaglutide for obesity treatment, patients saw a 17.3 kg reduction in body weight. Based on dual-energy X-ray absorptiometry scans, they also had a 6.9 kg mean reduction in total lean mass — which includes muscle. That means approximately 40% of the weight lost came not from fat, but from lean tissue.
A 2024 systematic review examining lean mass changes across multiple semaglutide clinical trials found that lean mass loss as a fraction of total weight lost ranged from approximately 25% to 60%. The range is wide because it varies by dose, age, baseline muscle mass, diet, and whether the person is exercising. But even at the lower end of that range, one in four kilograms lost is muscle — not fat.
Experts have noted that participants using semaglutide in 68 to 72-week clinical studies lost 10% or more of their muscle mass — roughly equivalent to 20 years of age-related muscle loss compressed into just over a year.
To be fair, the picture is not entirely alarming for younger, healthier adults. The body composition overall often improves on these drugs — less fat relative to lean mass — and for many patients, the metabolic benefits of losing significant fat outweigh the muscle loss concern. The drugs are doing what they are supposed to do.
But there is a specific population for whom this concern becomes clinically urgent: older adults, people already at low baseline muscle mass, and — as we have written about extensively — Indian bodies, which already carry less skeletal muscle relative to fat compared to other populations.
The Sarcopenia Problem — Accelerated

A 2025 retrospective cohort study followed older adults with type 2 diabetes on semaglutide over 24 months and found evidence of accelerated sarcopenia, particularly at higher doses and in individuals who already had low baseline muscle mass and reduced physical function. Semaglutide treatment significantly reduced both body mass index and muscle mass compared to controls. Grip strength initially improved but then declined, and gait speed reduced significantly in both men and women.
An editorial published in the Annals of Internal Medicine specifically warned that GLP-1 medications may exacerbate sarcopenia in older patients, noting that sarcopenic obesity — the combination of reduced muscle mass and excess fat — already affects an estimated 28.3% of people over age 60. These are precisely the people most likely to be prescribed these drugs.
Natural aging reduces skeletal muscle mass by 12 to 16% over a lifetime, leaving little margin before critical thresholds associated with frailty, fall risk, and functional impairment are crossed. Medication-induced muscle loss on top of this could push some patients over the edge.
And then there is the weight regain question. Research suggests that as much as two-thirds of weight lost on GLP-1 drugs may be regained after discontinuation. When lean mass is lost during treatment, the body may be less equipped to maintain results over time — because muscle is the primary driver of metabolic rate. Less muscle means slower metabolism. Slower metabolism means weight comes back faster and harder when the drug stops.
This is the cycle that concerns us.
Weight Loss Alone Is Not Wellness

We wrote previously about why protein alone cannot build muscle without the training signal. The same logic applies here — but in reverse.
Weight loss alone cannot deliver wellness without protecting muscle in the process.
The drugs may successfully reduce the risk of the most acute and deadly consequences of obesity — cardiovascular events, severe diabetes complications, organ damage from visceral fat. We acknowledge this sincerely. These are lives being saved, and that matters enormously in a country where these diseases are epidemic.
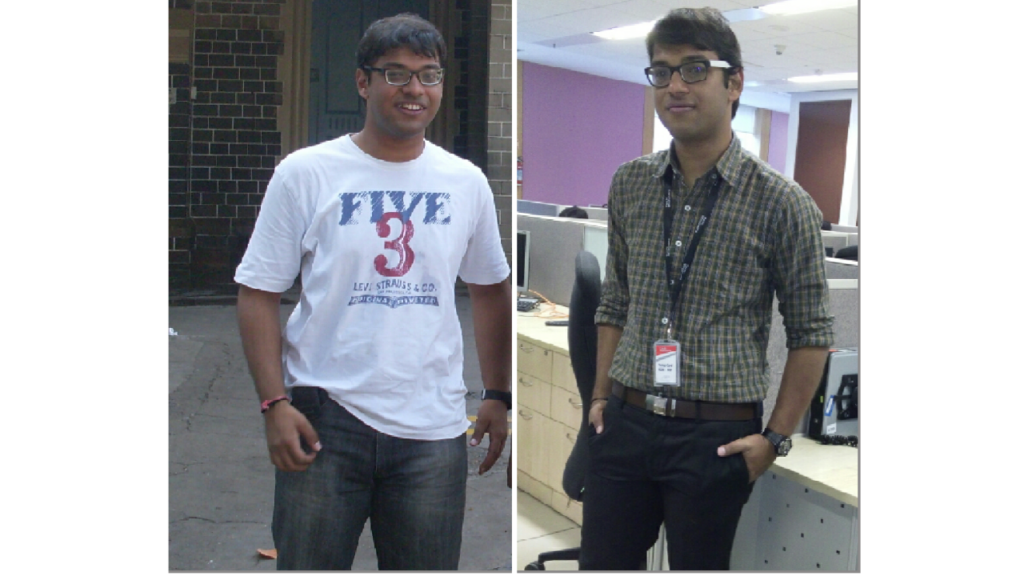
But weight, as we have argued before, is the wrong primary metric for health. What your body is made of matters more than what it weighs. A person who loses 15 kilograms on semaglutide but loses 6 of those kilograms as muscle has not simply become healthier — they have shifted their body composition in a direction that, if not actively countered, sets them up for the next problem: weaker muscles, slower metabolism, reduced quality of life, and — eventually — the accelerated biological ageing that comes from sarcopenia.
The goal is not to be thin. The goal is to be functional, metabolically healthy, and strong enough to live well for decades.
What You Need to Do Alongside These Drugs

The answer is not to avoid semaglutide if your doctor has prescribed it. The answer is to not treat it as a complete solution on its own.
The research is clear on what mitigates the muscle loss risk: two things, used together.
Structured resistance training. Your muscles need a signal that they are still needed. Without the mechanical stimulus of strength training, your body has no reason to preserve muscle during rapid weight loss — it will shed it as readily as fat. Exercise sends the signal. It tells your body: these muscles are in use, protect them.
Adequate protein intake. As we wrote in a previous blog, protein without training does not build muscle. But training without protein cannot repair the muscle tissue that exercise breaks down. Both are necessary. During a period of significant caloric reduction — which is exactly what semaglutide induces through appetite suppression — protein intake becomes even more critical, because the body is getting fewer total calories and needs to prioritise what it does receive.
In the absence of either, you will lose weight. But you will lose muscle alongside the fat, your metabolism will slow, and the weight loss — if it is ever interrupted or the medication is stopped — will return more aggressively than before.
The DashFit Perspective
We value the lives that GLP-1 drugs like Ozempic and Wegovy can potentially save — especially in India, where the scale of the metabolic disease crisis demands every effective tool available.
But a drug that reduces appetite and drives weight loss is addressing one variable. Your wellbeing depends on more than one variable.
It depends on what your body is made of. It depends on whether your muscles are receiving the signals they need to stay strong, functional, and metabolically active. It depends on whether the weight you are losing is predominantly fat — or whether you are quietly trading one problem for another.
This is precisely why DashFit starts with a body composition assessment, not a weight measurement. It is why every plan is built around muscle health — tracking which muscles are active, which are undertrained, and what stimulus they need week on week. It is why protein and structured strength training are not optional additions to a weight loss plan. They are the plan.
No matter what approach you take to lose weight — whether through medication, diet, or exercise — take deliberate steps to protect your muscle in the process.
Because the version of you that is lighter but weaker is not the version worth working toward.
Built for discipline. Powered by data. DashFit — Performance fitness for the modern professional.
Disclaimer: This blog is for informational purposes only and does not constitute medical advice. Please consult your doctor before starting or stopping any medication.